
Tuebingen
Techniques of 3D-Histology („Tuebinger Torte“ and „Muffin technique“)
Matthias Möhrle
Excision
„Tübinger Torte“ (Tuebingen Cake) and “Muffin Technique”
Intraoperatively a small incision or a suture is placed for topographical orientation, usually at 12:00 o’clock (most cranial point).
The tumor and the safety margin are removed en bloc. The incision is made perpendicularly to the surface of the skin which is preferable for defect closure.
Margin
„Tübinger Torte“ (Tuebingen Cake) and “Muffin Technique”
Using 3D-Histology the safety margin may range from 1 to 10 mm. The margin depends on various factors:
1. Tumour size. The larger a tumour the bigger a safety margin may be chosen to avoid multiple stages of excision.
2. Localisation. The delicate and aesthetically important the localision the smaller an initional safety margin will be chosen to spare healthy tissue.
3. Tumour type. An infiltrative tumour type justifies a larger initial safety margin.
Macroscopic preparation
„Tübinger Torte“ (Tuebingen Cake)
In 1984, this method was published by Breuninger and collegues (‘histologic control of excised tissue edges’) and later became popular under the name “Tübinger Torte”.
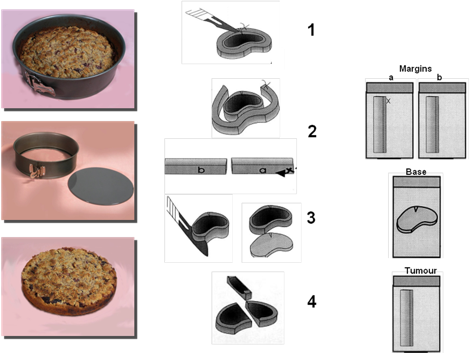
From the surgical specimen (tumour and safety margin excised en bloc) a narrow (1-2mm) lateral marginal strip is cut around the full perimeter of the tumour border, beginning with the above mentioned topographical mark at 12 o’clock. The strip is then laid flat on the peripheral side and cut into pieces which are placed in routine cassettes for histological evaluation (figure 1: 1 and 1).
Subsequently a horizontal section is cut from the bottom of the excised specimen and likewise prepared flat in a histology cassette (figure 1: 3).
Strips of the tumour are placed in histology cassettes as well (figure 1: 4). For topographical orientation dye marks can be used.
The method uses routine overnight paraffin fixation, thus reducing time and costs. The specimens, which may be fixed for 2 h in a formalin solution at 60 ° C, are available 20 h later, and provide a complete three-dimensional view of the excision margins.
Figure 1: “Tubinger Torte”
“Muffin Technique”
The Muffin technique had been refined and named Muffin technique by Moehrle & Breuninger in 2006; a similar technique (“Flunder Technik”) had been introduced by Breuninger & Holzschuh in 1994.
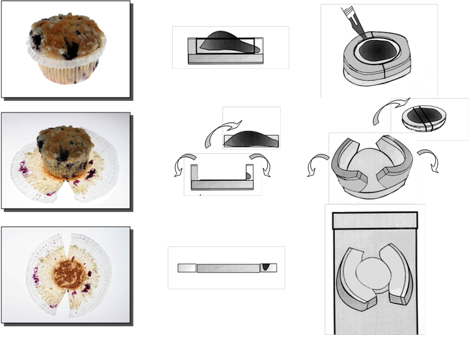
Deep incisions at 12 o’clock and 6 o’clock relative to the body axis are made.
Then a narrow lateral strip is cut without dissecting the base.
Using dissecting scissors the central part is removed without cutting into the base.
Similar to the peeling off of a muffin’s paper mould these margins can be folded laterally to a horizontal plane.
The specimen is placed in a routine cassette for horizontal fixation. For topographical orientation dye marks can be used.
The cassettes may be fixed for 2 h in a formalin solution at 60 ° C. Histological slides are available 20 h later, and provide a complete three-dimensional view of the excision margins of the tumour on one single slide.
The Muffin technique may be used for specimens up to 2 cm in diameter.
Figure 2: “Muffin Technique”
Similar to Mohs technique, it is not possible to evaluate the distance between the tumor and the incision margin neither using the “Tuebinger Torte” nor using the “Muffin technique”.
Indications
Common indications include basal cell carcinoma (especially infiltrative types), recurrent basal cell carcinomas, or neural infiltrating variants, as well as squamous cell carcinoma that have infiltrated the subcutis or have moderate to poor differentiation.
Dermatofibrosarcoma protuberans, lentigo maligna, lentigo maligna melanoma, acral lentiginous melanoma, and Merkel cell carcinoma are also indications as are erythroplasia of Queyrat, extramammary Paget disease, and Bowen’s disease. The paraffin section method is preferred in most cases, given then tumor extensions may be better evaluated than with cryostat procedures. This applies in particular to squamous cell carcinoma, Merkel cell carcinoma, and extramammary Paget’ disease. Micrographic surgery using paraffin sections is especially important for recurrent tumors, dermatofibrosarcoma protuberans, lentigo maligna melanoma, and acrolentiginous melanoma.
3D histology should be used for malignant tumors at critical sites or when it is expected that more complex closure techniques will be needed and thus complete tumor removal must be ensured prior to wound closure. The more problematic the tumor and the affected site, the more important is the choice of such a highly sensitive 3D histology to confirm free margins.
Continuous visualization of the lateral and basal margins, without any diagnostic gaps is independent of the diameter of the excised tumor.
In tumors that have infiltrated the bone, the procedure is of limited use. Osseous components might be decalcified and can then be histologically examined.
Literature
Breuninger H.
Histologic control of excised tissue edges in the operative treatment of basal-cell carcinomas.
J Dermatol Surg Oncol 1984; 10: 724–728
Möhrle M, Breuninger H.
The Muffin technique--an alternative to Mohs' micrographic surgery.
J Dtsch Dermatol Ges. 2006; 4: 1080-4
Moehrle M, Breuninger H, Rocken M.
A confusing world: what to call histology of three-dimensional tumour margins?
J Eur Acad Dermatol Venereol. 2007; 21: 591-5
Löser C, Rompel R, Breuninger H, Möhrle M, Häfner HM, Kunte C, Hassel J,
Hohenleutner U, Podda M, Sebastian G, Hafner J, Konz B, Kaufmann R.
Microscopically controlled surgery (MCS).